
Tags
cardiovascular disease, carotid artery, cerebrovascular disease, heart disease, Impacts of Radiation, ionizing radiation, no safe dose, NRC, nuclear energy, nuclear safety, nuclear workers, radiation, stroke, worker safety

The comment deadline is past, but the topic is still critically important. Some comments may be seen at the link. The US NRC Comment Deadline on “Radiation Protection” ended Monday 22 June 2015. Uploaded comments may be seen here: http://www.regulations.gov/#!documentDetail;D=NRC-2009-0279-0098 (ID: NRC-2009-0279-0098)
The original list of questions to be answered is found here. It is now difficult to find: https://www.federalregister.gov/articles/2014/07/25/2014-17252/radiation-protection There have been several extensions so it may have been accidentally quasi lost (or not).
http://www.regulations.gov/#!documentDetail;D=NRC-2009-0279-00670
The presentation of questions is indicative of someone who is heartless or with a heart of stone. They show no concern for worker safety, nor for the unborn child, whose mother works with radiation. So, forgetting risk of cardiovascular and cerebrovascular should not be surprising.
The US NRC is ignoring the “findings” of the ICRP 118 regarding cardiovascular and cerebrovascular disease and only discussing the new ICRP “findings” re cataract risk and a few more safety related issues, which the US NRC doesn’t seem very interested in implementing.
The ICRP says: “… a ‘threshold dose’ of 0.5 Gy is proposed here for both cardiovascular disease and cerebrovascular disease on the basis that this dose might lead to approximately 1% of exposed individuals developing each disease in question. Nevertheless, there are notable uncertainties in determining risks of these diseases at this level of dose.” (p.292)
“An approximate threshold dose of around 0.5 Gy has been proposed for acute and fractionated/protracted exposures, on the basis that this might lead to circulatory disease in only one to a few percent of exposed individuals, although the estimation of risk at this level of dose is particularly uncertain.” p. 304, ICRP 118.
This is essentially 500 mSv, meaning that with the current 50 mSv per year worker dose, over a 10 year period, there would be a 1% to 2% excess relative risk of cardiovascular or cerebrovascular disease among workers. Over 40 years it would be 4 to 8 %. On one page they imply that this is mortality and that morbidity (illness) would be greater. At the 20 mSv per year (100 mSv for 5 yrs with no year higher than 50 mSv) proposed by the ICRP since 1991, and begrudgingly raised as a possibility by the US NRC, the 500 mSv would be reached after 25 years. This really suggests need of a maximum exposure of 10 mSv or less for workers.
This is also apparently for external exposure and, thus, ignores that cesium and strontium would act as chemical, along with radiological, poisons, by acting as mimics to potassium and calcium, both required for heart function (as well as for the entire nervous system and non-cardiac muscles).
IRCP 118, Summary:
“ICRP Statement on Tissue Reactions / Early and Late Effects of Radiation in Normal Tissues and Organs – Threshold Doses for Tissue Reactions in a Radiation Protection Context ICRP Publication 118 Ann. ICRP 41(1/2), 2012, by F.A. Stewart, A.V. Akleyev, M. Hauer-Jensen, J.H. Hendry, N.J. Kleiman, T.J. MacVittie, B.M. Aleman, A.B. Edgar, K. Mabuchi, C.R. Muirhead, R.E. Shore, W.H. Wallace
Abstract – This report provides a review of early and late effects of radiation in normal tissues and organs with respect to radiation protection. It was instigated following a recommendation in Publication 103, and it provides updated estimates of ‘practical’ threshold doses for tissue injury defined at the level of 1% incidence. Estimates are given for morbidity and mortality endpoints in all organ systems following acute, fractionated, or chronic exposure. The organ systems comprise the haematopoietic, immune, reproductive, circulatory, respiratory, musculoskeletal, endocrine, and nervous systems; the digestive and urinary tracts; the skin; and the eye.
Particular attention is paid to circulatory disease and cataracts because of recent evidence of higher incidences of injury than expected after lower doses; hence, threshold doses appear to be lower than previously considered. This is largely because of the increasing incidences with increasing times after exposure. In the context of protection, it is the threshold doses for very long follow-up times that are the most relevant for workers and the public; for example, the atomic bomb survivors with 40–50 years of follow-up. Radiotherapy data generally apply for shorter follow-up times because of competing causes of death in cancer patients, and hence the risks of radiation-induced circulatory disease at those earlier times are lower.
A variety of biological response modifiers have been used to help reduce late reactions in many tissues. These include antioxidants, radical scavengers, inhibitors of apoptosis, anti-inflammatory drugs, angiotensin-converting enzyme inhibitors, growth factors, and cytokines. In many cases, these give dose modification factors of 1.1–1.2, and in a few cases 1.5–2, indicating the potential for increasing threshold doses in known exposure cases. In contrast, there are agents that enhance radiation responses, notably other cytotoxic agents such as antimetabolites, alkylating agents, anti-angiogenic drugs, and antibiotics, as well as genetic and comorbidity factors.
Most tissues show a sparing effect of dose fractionation, so that total doses for a given endpoint are higher if the dose is fractionated rather than when given as a single dose.” [Comment: This is only true if repair is adequate.]
“However, for reactions manifesting very late after low total doses, particularly for cataracts and circulatory disease, it appears that the rate of dose delivery does not modify the low incidence.
This implies that the injury in these cases and at these low dose levels is caused by single-hit irreparable-type events. For these two tissues, a threshold dose of 0.5 Gy is proposed herein for practical purposes, irrespective of the rate of dose delivery, and future studies may elucidate this judgement further.” “ICRP, 2012 ICRP Statement on Tissue Reactions / Early and Late Effects of Radiation in Normal Tissues and Organs – Threshold Doses for Tissue Reactions in a Radiation Protection Context. ICRP Publication 118. Ann. ICRP 41(1/2).”
http://www.icrp.org/publication.asp?id=ICRP%20Publication%20118
(Emphasis our own)
Comment: Obviously it is caused by one, or more, un-repaired hits! That’s the nature of ionizing radiation! This suggests that it could happen at any dose. Or, perhaps, it is an accumulation of un-repaired or mis-repaired damage, at least for cataracts.
Now ICRP 118 is made available in Chinese for free too by the ICRP, along with Russian: https://miningawareness.wordpress.com/2014/11/20/us-nrc-comment-extension-needed-info-only-in-russian/ The important 2007 ICRP 103 document, referred to above, is available in almost every language BUT English.
The US NRC finally made ICRP 118 available, probably due to formal public complaints. If you read neither Chinese, nor Russian, hard copies may be had for $362.00 or roughly a dollar per page.
Type ML13269A319 to obtain it online from the US NRC:
“(678) Circulatory disease has not previously been listed by ICRP as a health hazard from radiation exposures to organs and tissues, because it is only in the last few years that there has been greater consolidation of the evidence on this topic. This includes heart disease arising >10 years after irradiation from atomic bombs or after the Chernobyl accident, or after irradiation of a part of the heart during radiotherapy for breast cancer, peptic ulcer, or Hodgkin’s lymphoma….” (p. 290)
“…it is unclear whether there is a dose below which the risk of circulatory disease is not increased and, if so, what this dose might be. Nevertheless, based on the epidemiological findings, it is possible to estimate the magnitude of dose at which circulatory disease might be induced among 1% of exposed individuals…
If an ERR/Gy of this magnitude were to apply at doses in the range of 0.5 Gy, and the baseline incidence is 30–50%, this would imply that a dose of 0.5 Gy might increase mortality from circulatory disease by approximately 0.08 · 0.5 · (30–50)% = 1.2–2%. Given that not all cases of circulatory disease are fatal, the corresponding percentage for morbidity would be expected to be greater. Overall, and subject to the assumptions outlined here, a dose of around 0.5 Gy might lead to approximately 1% of exposed individuals developing circulatory disease.” (pp. 291-292)
“(683) It is unclear from Table 2.4 whether the ERR/Gy for cardiovascular disease is greater than that for cerebrovascular disease. In a recent report (Table 8 in AGIR, 2010), the aggregate ERR/Gy from many appropriate studies was estimated to be 0.09 (95% CI 0.05–0.12) for cardiovascular disease and 0.21 (95% CI 0.16–0.27) for cerebrovascular disease. However, around a potential threshold dose of 0.5 Gy, this difference is uncertain. On the basis that the baseline risk for cardiovascular disease (e.g. around one in six deaths in the UK – AGIR, 2010) is greater than that for cerebrovascular disease (around one in nine of deaths in the UK – AGIR, 2010), then as the ERR/Gy may be greater for cerebrovascular disease than for cardiovascular disease, a ‘threshold dose’ of 0.5 Gy is proposed here for both cardiovascular disease and cerebrovascular disease on the basis that this dose might lead to approximately 1% of exposed individuals developing each disease in question. Nevertheless, there are notable uncertainties in determining risks of these diseases at this level of dose.” (p.292)
[…]
“(685) It is unclear whether or not the ERR/Gy is the same for acute, fractionated, and chronic exposures. Similar threshold doses would be expected in these three conditions if the risk at doses up to the threshold dose were governed by single-hit irreparable injury, with no split-dose repair, slow repair, or cell repopulation effect involved at these very low dose levels. However, the problem for the present purpose is the difficulty of determining the threshold dose to a good degree of accuracy in different human exposure scenarios, and the much discussed likelihood of the mechanism of circulatory disease being different at high vs low doses. If the mechanisms are different, it is probably fortuitous that threshold doses are considered similar for acute, fractionated, or chronic exposures, and statistical uncertainties are reflected in this choice. For the purposes of the present assessment, the ERR/Gy and hence the ‘threshold dose’ is taken to be the same for all three types of exposure, i.e. around 0.5 Gy. Future studies may elucidate this further.” (p. 292)
“(711) This report has produced some changes to indicated threshold doses for tissue reactions (see Tables 4.4 and 4.5) compared with those stated in Publication 103 (ICRP, 2007). First, the threshold dose for radiation-induced eye cataracts is now considered to be around 0.5 Gy for both acute and fractionated/chronic exposures, in line with various recent epidemiological studies. Second, circulatory disease has been recognised as an important late effect of radiation exposure, both for mortality and morbidity. An approximate threshold dose of around 0.5 Gy has been proposed for acute and fractionated/protracted exposures, on the basis that this might lead to circulatory disease in only one to a few percent of exposed individuals, although the estimation of risk at this level of dose is particularly uncertain.” (p. 304)
“(712) Third, the threshold dose values for chronic exposures depend on the exposure duration and the follow-up period after exposure. Differences between these time variables among different studies make the values more uncertain. The values quoted for both the lens and the circulatory system assume the same incidence of injury irrespective of the acute or chronic nature of the exposure over a working life, with >20 years follow-up. Future studies may elucidate this further. For the public, the annual threshold dose values would be scaled down in proportion to relative life span minus latency period (20 years latency for lens, 10 years for circulatory disease) vs working life. It is emphasised that great uncertainty is attached to these values.” (p. 305) – ICRP 118
So after retirement you don’t have to be able to see? Am I missing something here?
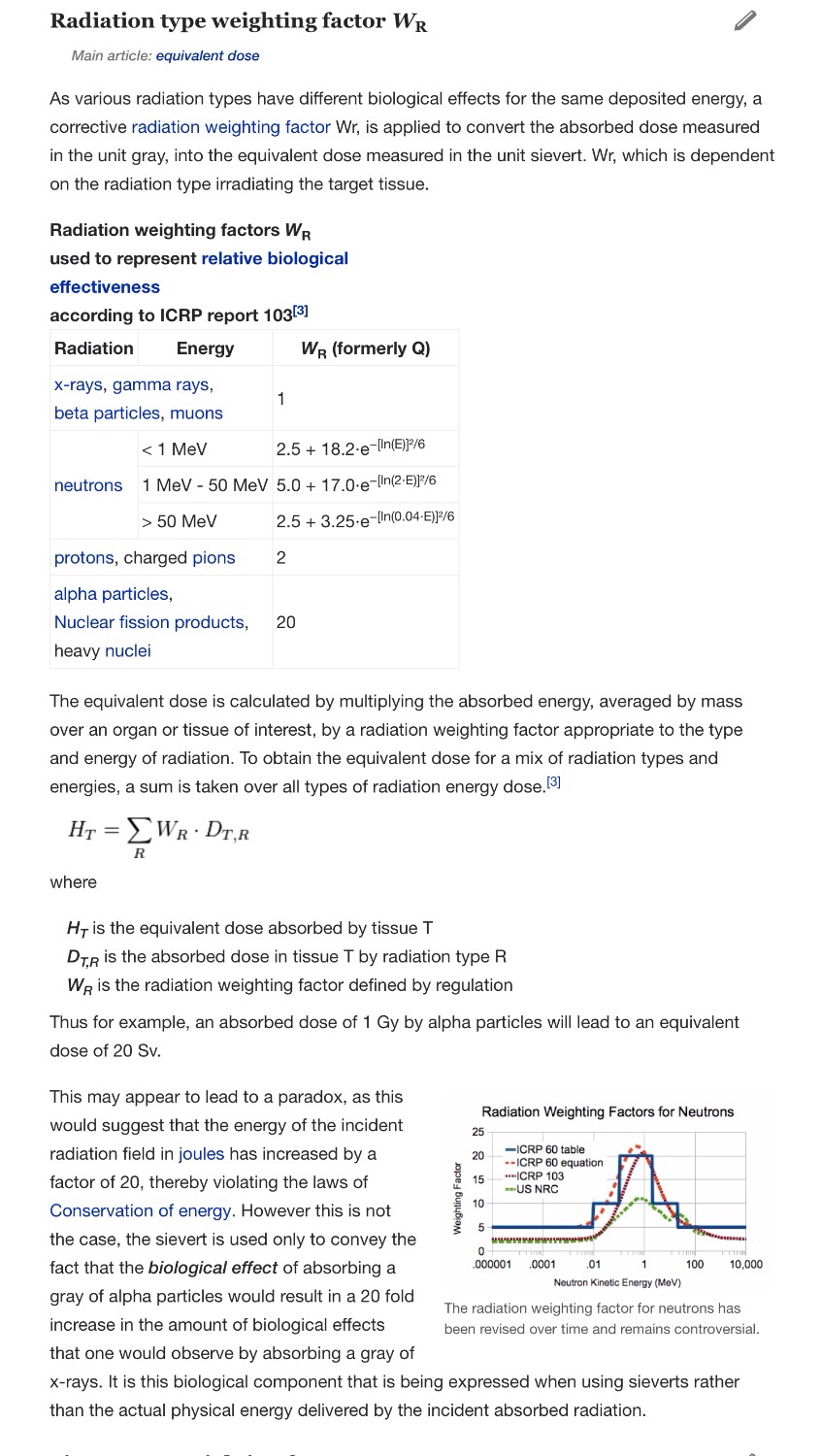
Sieverts and their Relationship to Grays
Since the ICRP is basing its findings mostly on external, low LET, radiation, mGy and mSv would be essentially the same. It is, in fact, dangerous to use Gray, because, as explained below, one Gray of plutonium would be 20 Sieverts.
“The sievert (symbol: Sv)[note 1] is a derived unit of ionizing radiation dose in the International System of Units (SI). It is a measure of the health effect of low levels of ionizing radiation on the human body. Quantities that are measured in sieverts are intended to represent the stochastic health risk, which for radiation dose assessment is defined as the probability of cancer induction and genetic damage.[1]
The sievert is used for radiation dose quantities such as equivalent dose, effective dose, and committed dose. It is used both to represent the risk of the effect of external radiation from sources outside the body, and the effect of internal irradiation due to inhaled or ingested radioactive substances.
Conventionally the sievert is not used for high levels of radiation which produce deterministic effects, which is the severity of acute tissue damage which is certain to happen. These effects are compared to the physical quantity absorbed dose measured by the unit gray (Gy).[2]
To enable consideration of stochastic health risk, calculations are performed to convert the physical quantity absorbed dose into equivalent and effective doses, the details of which depend on the radiation type and biological context. For applications in radiation protection and dosimetry assessment the International Commission on Radiological Protection (ICRP) and International Commission on Radiation Units and Measurements (ICRU) have published recommendations and data which are used to calculate these.
The sievert is of fundamental importance in dosimetry and radiation protection, and is named after Rolf Maximilian Sievert, a Swedish medical physicist renowned for work on radiation dosage measurement and research into the biological effects of radiation… Doses greater than 1 sievert received over a short time period are likely to cause radiation poisoning, possibly leading to death within weeks.
One sievert equals 100 rem. The rem is an older, non-SI unit of measurement.
To enable a comprehensive view of the sievert this article deals with the definition of the sievert as an SI unit, summarises the recommendations of the ICRU and ICRP on how the sievert is calculated, includes a guide to the effects of ionizing radiation as measured in sieverts, and gives examples of approximate figures of dose uptake in certain situations….”
https://en.wikipedia.org/?title=Sievert
Weighting factors are of critical importance for defining what is considered safe. Also, dose coefficients are very important for ingestion, inhalation and absorption. Apparently small numerical changes make big differences so they are easily manipulated.
It now is believed that the RBE for tritium should be two or three:
“There is growing evidence to support a relative biological effectiveness (RBE) greater that one for low-energy electrons and photons. Strong justification of an RBE greater than one for low energy electrons comes from radiobiological studies of tritium…. Low-energy electron and photon radiations produce dense ionization clusters which lead to RBE values greater than those of high energy gamma rays. For tritium, RBE values between 2 and 3 are implied by a number of experimental studies. Other radiation sources with similar energy emissions may also exhibit an elevated RBE.” (Oak Ridge National Lab for the US EPA, 2013)
“RBE and wR values of Auger emitters and low-range beta emitters with particular reference to tritium” by Ian Fairlie 2007, “Journal of Radiological Protection “Volume 27 Number 2 Received 1 June 2005, accepted for publication 27 January 2007. Published 25 May 2007. IOP Publishing Ltd
“Abstract
An apparent disparity exists between RBE (relative biological effectiveness) values for low-range beta and Auger emitters, and the current value for their radiation weighting factor (wR). This paper presents evidence that the current wR value of unity for these nuclides is inconsistent with most RBE evidence and should be increased by a factor of two to three. It recommends that the ICRP should clearly state that the most appropriate RBE value for these nuclides, and not the wR value, should be used in specific dose calculations, retrospective dose estimations and epidemiological studies. The ICRP should also publish guidance as to the methods and data sources that could be used for these RBE values.”
Also see: http://www.icrp.org/consultation_viewitem.asp?guid=%7B1DAF74F3-05CB-43A7-96CE-E296E0FF061E%7D

You must be logged in to post a comment.